Effects on the anterior eye segment when docking a femtosecond laser to the patient interface
Purpose: Ziel der Studie war der Vergleich des intraoperativen OCT (optischen Kohärenztomographen) des LenSx Femtosekundenlasers (Alcon Pharma GmbH, Freiburg) mit einem To compare the intraoperative OCT (optical coherence tomographer) of the femtosecond laser LenSx (Alcon Pharma GmbH, Freiburg) with a Scheimpflug-tomographer and an anterior segment OCT and thus to investigate a possible influence on the anterior segment of the eye when docking the patient’s interface.
Material and Methods: A prospective cross-sectional study was conducted with 57 subjects who underwent a planned femtosecond laser-assisted cataract surgery or refractive lens exchange. The eye to be operated on was measured prior to the operation in mydriasis with the Visante OCT (Carl Zeiss Meditec AG, Jena) and the Pentacam AXL (Oculus Optikgeräte GmbH, Wetzlar). During the surgery, images of the anterior segment of the eye were taken by the integrated intraoperative OCT of the laser, which were evaluated afterwards and compared to the values of the other devices. The parameters examined were the internal anterior chamber depth (ACD), nasal and temporal chamber angles, central corneal thickness (CCT) and central lens thickness (LT).
Results: The comparison of the intraoperative OCT and the two other devices showed clinically relevant differences in all parameters. The intraoperative OCT showed a 9.19 ± 27.55 μm larger CCT, 0.96 mm (median difference) larger LT, 0.05 mm smaller ACD than the Pentacam AXL and a 21.36 ± 25.50 μm larger CCT, 0.10 mm (median difference) smaller ACD than
the Visante OCT.
Conclusion: The comparison of the intraoperative OCT with the Visante OCT and the Pentacam AXL shows clinically relevant differences. Changes in the anterior segment of the eye may be due to errors in measurement or docking of the patient’s interface.
Introduction
In recent years, the use of femtosecond lasers has become a usual practice in the field of ophthalmic surgery.1 In surgical interventions such as cataract surgery, the femtosecond laser carries out important surgical steps such as making the incisions in the cornea, the capsulorrhexis and fragmenting the lens of the eye.2 For a femtosecond laser to function, it is necessary to establish contact with the cornea so as not to allow any air between the laser and the section plane.3 The LenSx® femtosecond laser from Alcon Pharma GmbH (Freiburg) uses a rigid, curved patient interface for this purpose, which is placed in combination with a special soft contact lens that lies between the interface and the cornea.4 The docking process is transferred to a screen in real time via an integrated optical coherence tomograph (OCT) and is therefore carried out in a controlled manner.4 With the help of the integrated OCT, the incisions in the cornea and the position of the capsulorrhexis as well as the karyorrhexis of the lens are then precisely planned.4
However, the validity of the measurement data of the integrated intraoperative OCT as well as the effects of the docking process on the anterior eye segment and its possible influence on the measurement results have not yet been investigated. The aim of this study is to compare the measurement results of the intraoperative OCT with those of other devices, and thus to examine a possible influence of the docking process of the patient interface on the anterior eye segment. For this purpose, the measurement data of the internal anterior chamber depth, the nasal and temporal chamber angles as well as the central corneal and lens thickness obtained by the integrated intraoperative OCT of the LenSx® laser were compared with the measurement data of the anterior segment OCT Visante™ from Carl Zeiss Meditec AG (Jena) and the Scheimpflug tomograph Pentacam® AXL from Oculus Optikgeräte GmbH (Wetzlar).
Material and Methods
A prospective, monocentric cross-sectional study was carried out in the eye clinic of the University Hospital in Frankfurt am Main. Healthy test subjects over the age of 18 who were about to have a scheduled femtosecond laser-assisted refractive lens exchange, or a femtosecond laser-assisted cataract operation were included in the study. Corneal pathologies and previous anterior eye segment or refractive surgeries were considered exclusion criteria. Only one eye was measured per patient. In order to randomise the study, the eye that was operated on first was chosen for the study.The study was checked and approved by the ethics committee of the medical department of the Goethe University Hospital in accordance with professional law and ethical guidelines.
It complies with the principles of the Declaration of Helsinki and we applied the guidelines of Good Clinical Practice (GCP). Before the patients were included in the study, they were given a detailed explanation by the study physician about the purpose, procedure and risks of participating in it. All patients received patient information, signed a declaration of consent and thus consented to the use of their anonymised data in the context of the study. For anonymisation purposes, each test subject was given a specific number.
We carried out a sample size planning with the statistics program BIAS for Windows in cooperation with the biometric consultancy of the University Hospital Frankfurt in order to determine the necessary sample size for the study. The level of significance was set at α = 0.05, and a statistical power of 0.8 was required. The study by Shajari et al. (2016)5 assumed a maximum permissible difference between the Visante™ and Pentacam® procedures, up to which there is no difference between the two, of around half a standard deviation for the sample size calculation. This corresponds to an average effect for the allowable difference. Based on these assumptions, a minimum of 36 patients must be included in the study in order to be able to demonstrate the equivalence of two procedures with the one-sample t-test at a significance level of 5% and a statistical power of 80%. Assuming a drop-out rate of 10%, at least 40 patients should be included in the study.
Procedure and Apparatus
The study-specific measurements were carried out in one examination room by only one examiner. The same apparatus were always used for the measurements and their position was not changed. The sequence of measurements was determined at the beginning of the study and followed throughout (first Pentacam® AXL, then Visante™ OCT, followed by surgery with the LenSx® femtosecond laser). The study-specific examinations and the operation with the LenSx® femtosecond laser were both carried out in mydriasis. The manual measurement of the OCT images, both of the anterior segment OCT and of the intraoperative OCT of the LenSx® femtosecond laser, was carried out by just one examiner in order to ensure a consistent procedure.
The data was collected by the Pentacam® AXL with software version 1.20b 119. The setting "3D scan / 25 images / 1 sec" was selected, the measurement was started in automatic mode and three measurements were performed out of which at least two showed no error message displayed by the software of the Pentacam® AXL in the field "QS" (quality specification).
The measurement was then carried out on the Visante™ OCT optical coherence tomograph with software version 3.0.1.8. An "AC Biometry PreOP" scan in 0°/180° was performed three times for each patient and the "Enhanced Anterior Segment Single" image was measured manually with the tools "ACAngle-180°", "ACAngle-0°" and "Chamber".
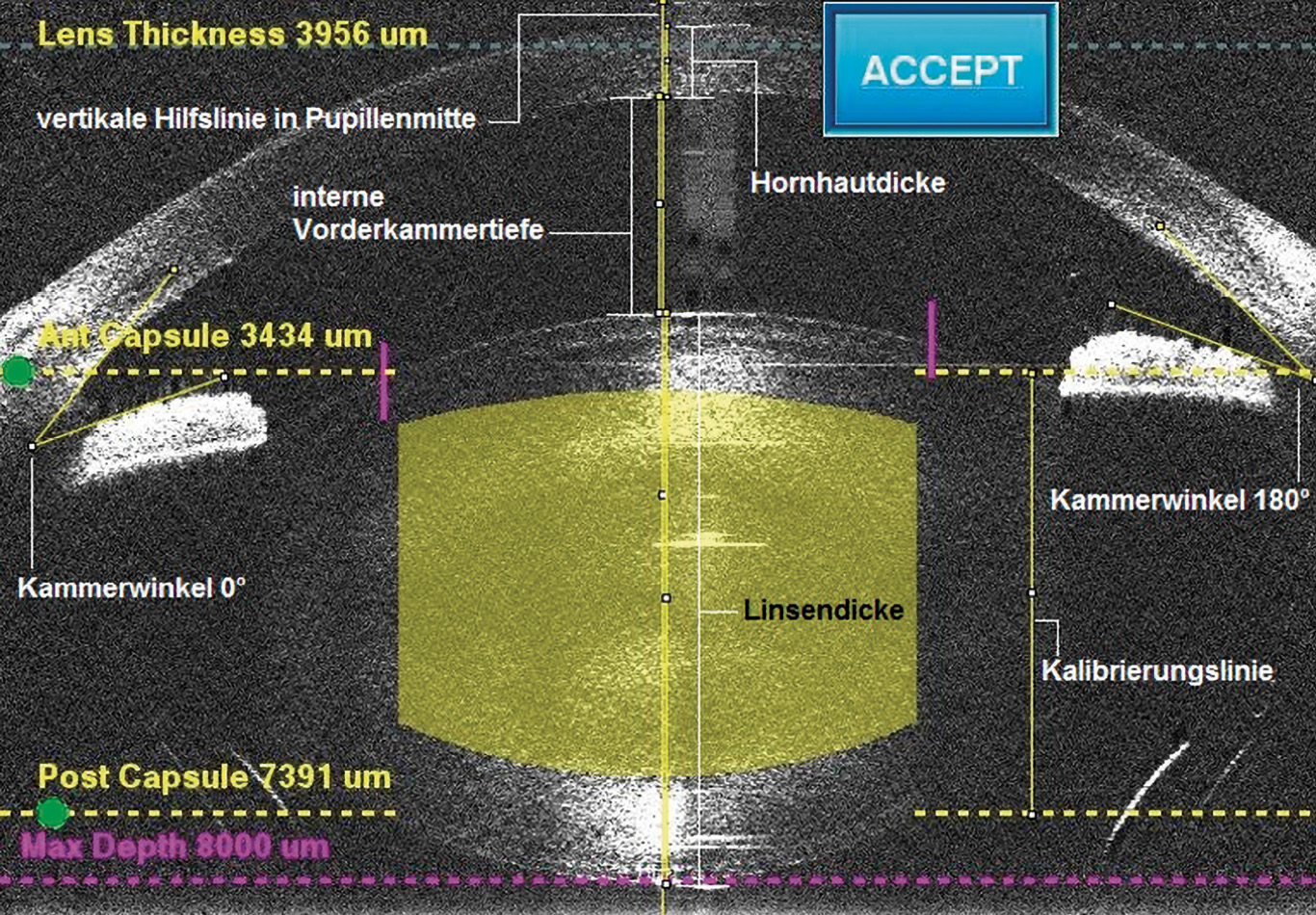
During the subsequent operation with the LenSx® femtosecond laser, various images of the intraoperative OCT were automatically saved, including images of the anterior eye segment in 0°/180° as a sectional image. A freely available image editing and processing program called fiji (fiji is just ImageJ), version 2.0.0, was used to measure these images. A macro was programmed for use on the OCT images, with which all relevant parameters could be measured manually in a pre-established order (Fig. 1).
Statistical analysis
Mean values were calculated from the data in Microsoft Excel for the statistical evaluation of the three or at least two measurements on the Pentacam® AXL and the Visante™ OCT. All data were transferred from Microsoft Excel to BIAS 11.04 for Windows. The Bland-Altman analysis was used to compare the methods. The differences in the measured values must be normally distributed in order to interpret the Bland-Altman analysis. These values were thus checked for Gaussian distribution using the Kolmogoroff-Smirnoff-Lilliefors test. The Wilcoxon matched pairs test was used for measured values that were not normally distributed. In order to be able to make a statistical statement about the difference between two methods, an equivalence range was defined as the maximum permissible difference which can be considered as not clinically relevant. If the 95% confidence interval for the mean difference (Bland-Altman analysis comparison) or the median difference (Wilcoxon matched pairs test) is within the specified equivalence range, the procedures can be regarded as equivalent. The deviation of the measured values was determined on the basis of a meta-analysis according to Rozema et al. (2014)6 to be ± 8.12 µm for the central corneal thickness and ± 0.085 mm for the internal anterior chamber depth. The tolerance value for the internal anterior chamber depth was transferred to the lens thickness and was thus also ± 0.085 mm since both values are given in mm and are of comparable size. The deviation of the chamber angles was determined to be clinically irrelevant at ± 5°, since the next degree of classification according to the Shaffer classification for chamber angles is only reached with a difference of 10°.7 Lin’s concordance correlation coefficient was used to examine the correlation between the measurement methods.
Results
57 test subjects with an average age of 66.16 ± 10.97 years were included in the study (max. 88 years, min. 36 years), 40 of the subjects were male, 17 were female. Only one eye per patient was included in the study; 26 were right eyes and 31 were left eyes. Of the 57 subjects, cataract surgery was performed in 48 cases and refractive lens exchange in 9 cases. 14 subjects were excluded from the evaluation for technical reasons or due to lack of time. The lens thickness could only be measured with the Pentacam® AXL and the intraoperative OCT of the LenSx® femtosecond laser, since on the Visante™ OCT in the setting "Enhanced Anterior Segment Single" only the front surface of the eye lens is visible and, therefore, several images would have had to be taken. This would have exceeded the time frame of the study. No lens thickness could be determined with the Pentacam® AXL in seven test subjects. In six cases, the lens thickness was only determined in one or two of the three measurements; in these cases, the existing measurement data were used for further evaluation. The chamber angle images of the Pentacam® AXL were checked for plausibility by three independent people. Images with unrealistic chamber angle positions or missing chamber angles were removed from the database (eight test subjects), or the mean values were corrected (five test subjects). The evaluation of the chamber angles was carried out with the values of the Pentacam® AXL without a plausibility check and with the corrected values..
Internal anterior chamber depth
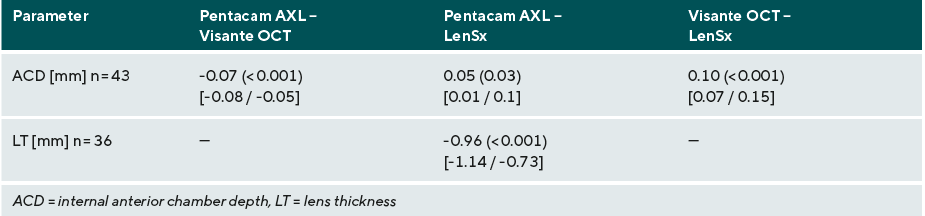
The median differences in the internal anterior chamber depth (ACD) of 0.05 mm (Pentacam® AXL - LenSx®) with p = 0.03 and 0.10 mm (Visante™ OCT - LenSx®) with p < 0.001 are each statistically significantly different, the 95% confidence intervals are not in the specified equivalence range of ± 0.085 mm, so the devices can be considered to be clinically different (Table 1).
Nasal and temporal chamber angles
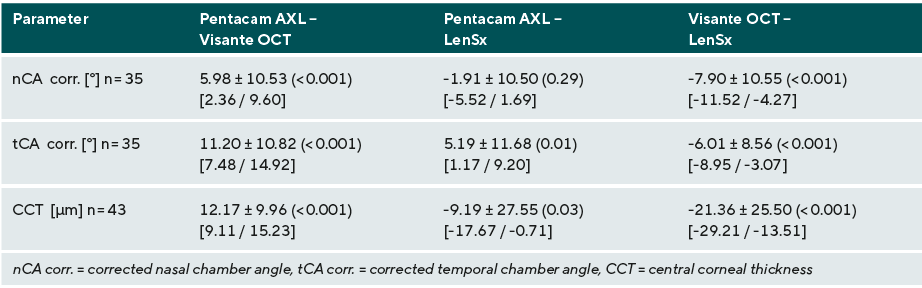
The measured values for the nasal chamber angles (nCA corr.) were checked for plausibility and then corrected. These showed a mean difference of -7.90 ± 10.55° (Visante™ OCT - LenSx®) with p < 0.001 and therefore exhibit a statistically significant and clinically relevant difference (Table 2). The comparison of Pentacam® AXL and LenSx® shows a mean difference of -1.91 ± 10.50° and an insignificant p-value of 0.29 for the corrected nasal chamber angles, but the results still exhibit a clinically relevant difference (Table 2).
The corrected temporal chamber angles (tCA corr.) show mean differences of 5.19 ± 11.68° (Pentacam® AXL - LenSx®) and -6.01 ± 8.56° (Visante ™ OCT - LenSx®) and significant p-values of 0.01 and <0.001. These results also differ in a clinically relevant manner (Table 2).
Central corneal thickness
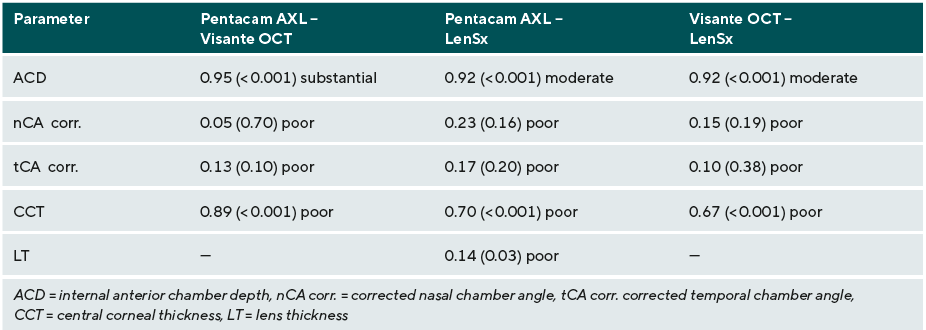
The central corneal thickness (CCT) values show a mean difference of -9.19 ± 27.55 µm (p = 0.03) between Pentacam® AXL and LenSx® and -21.36 ± 25.50 µm (p < 0.001) between Visante™ OCT and LenSx®. The 95% confidence intervals of the mean differences lie outside the clinically irrelevant equivalence range of ± 8.12 µm, so that the methods cannot be regarded as equivalent (Table 2). Lin's concordance correlation coefficients of 0.70 (Pentacam® AXL - LenSx®) and 0.67 (Visante™ OCT - LenSx®) indicate a correlation between the measured values (Table 3).
Central lens thickness
A median difference of -0.96 mm (Pentacam® AXL - LenSx®) with a significant p-value of p < 0.001 was obtained for the lens thickness (LT). The results differ in a clinically relevant manner (Table 1).
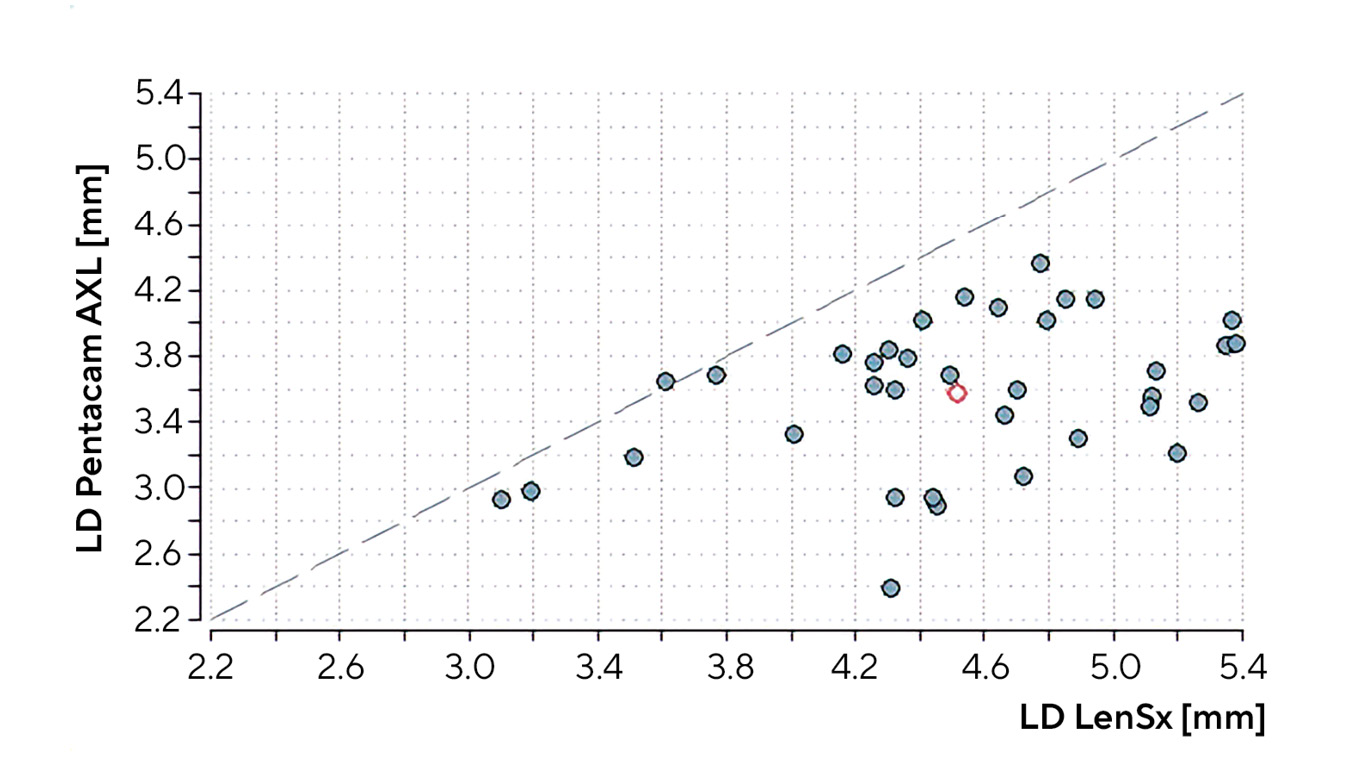
The p-value of 0.03 (Pentacam® AXL - LenSx®) for Lin's concordance correlation coefficient is also significant, but a Lin's rho of 0.14 is considered "poor" according to McBride (Table 3, Fig. 2).
Discussion
The aim of the study was to compare the results of the intraoperative OCT of the LenSx® femtosecond laser with the images of the Scheimpflug tomograph Pentacam® AXL and those of the anterior segment OCT Visante™ in order to investigate a possible influence on the anterior eye segment when the patient interface of the laser is docked.
Internal anterior chamber depth
If the ACD, measured with the intraoperative OCT of the LenSx® femtosecond laser, is compared with the results of the other two devices, this comparison shows a clinically relevant difference. The median differences were 0.05 mm (Pentacam® AXL - LenSx®, mean difference 0.06 ± 0.17 mm) and 0.10 mm (Visante™ OCT - LenSx®, mean difference 0.11 ± 0.13 mm). These values show that the intraoperative OCT of the LenSx® femtosecond laser measures a smaller ACD than the Pentacam® AXL and Visante™ OCT.
One possible explanation for this is that the pressure on the anterior segment of the patient's eye when the patient interface of the LenSx® femtosecond laser is docked causes a change in the shape of the anterior chamber. This results in a mean reduction in the internal anterior chamber depth of 50 µm compared to the Pentacam® AXL and of 100 µm compared to the Visante™ OCT.
A reduced ACD when applying suction to the patient's eye was already observed in 2009 by Kunert et al.8 In said study, the suction process of a similar patient interface (VISUMAX, Carl Zeiss Meditec AG, Jena) applied on a seated test subject was documented with the Visante™ OCT. A reduction of the ACD of 70 µm was found.8 A changed internal anterior chamber depth can also be the result of a modification of the corneal radii. During the docking process of the femtosecond laser, the patient's cornea is pressed against a rigid, curved patient interface with a soft contact lens (SOFTFIT™, Alcon) and adapts to the given curvature. If the radius of the interface is smaller than that of the cornea, it steepens and increases the ACD. If the radius of the interface is larger than that of the cornea, it will flatten and decrease the ACD.8
Nasal and temporal chamber angles
The interpretation of the differences in the measurement of the nasal and temporal chamber angles turned out to be difficult at first. The automatic chamber angle detection of the Pentacam® AXL worked well in most cases, but some chamber angles were not recognised or were identified incorrectly. For this reason, the images had to be checked for plausibility in order to obtain a meaningful result. Only the corrected chamber angles of the Pentacam® AXL, checked for plausibility, were used to interpret the results. This correction made it possible to greatly reduce the spread of the measured values, but the data still display a very wide scatter, and no correlation could be established between the measured values. As a result, no quantitative statement can be made about the possible effects of docking the LenSx® femtosecond laser to the patient's eye on the nasal and temporal chamber angles. However, there are clearly statistically and clinically relevant differences in the measurements between the devices.
One reason for the strong scatter of the measured values with the Pentacam® AXL, despite the correction, is the sensitivity of the internal software for chamber angle detection. Especially with light irises, there is often scattered light and overexposure around the limbus, making it difficult, if not impossible, to identify the chamber angle.9 The deepest point of the chamber angle cannot be determined exactly and the tangents on the posterior surface of the cornea and the anterior surface of the iris are incorrectly specified.
However, the evaluation of the images from the Visante™ OCT and the intraoperative OCT should also be analysed critically. The chamber angles were set manually for each image and are thus subject to the subjectivity of the examiner. The dispersion of the chamber angles of the intraoperative OCT was even higher in the case of low-contrast or very limited images. In these images, the deepest point of the chamber angle is difficult to see, which creates uncertainty in the positioning of the angle.
Central corneal thickness
The comparison of the central corneal thickness showed significant and clinically relevant differences between the devices. The mean differences were -9.19 ± 27.55 µm for Pentacam® AXL and LenSx®, and -21.36 ± 25.50 µm for Visante™ OCT and LenSx® (Table 2). The standard deviations of ± 27.55 µm and ± 25.50 µm indicate a rather large spread of the measured values for this parameter. The comparison of Pentacam® AXL and Visante™ OCT showed a significantly lower standard deviation of ± 9.96 µm, but the result is still clinically relevant with a mean difference of 12.17 µm (Table 2). In the meta-analysis by Rozema et al. (2014), the authors also describe a clinically relevant difference between Pentacam® and Visante™ OCT: The Scheimpflug tomograph measures a 13.57 ± 3.75 µm greater central corneal thickness than the OCT.6 In a 2017 study, Krysik et al. found a small but statistically significant difference between Pentacam® HR (552 ± 25 µm) and Visante™ OCT (550 ± 24 µm) in the measurement of the central corneal thickness.10 If this study is considered using a tolerance range for the mean difference of ± 8.12 µm, this result is not clinically relevant.
The results show that the intraoperative OCT of the LenSx® femtosecond laser measures a greater central corneal thickness than the other two devices. This could be due to the fact that the images of the intraoperative OCT were measured manually with the aid of a program based on the number of pixels. The central corneal thickness of the images from the Pentacam® AXL and Visante™ OCT was automatically determined by the internal software of the devices, whereby better resolution and image quality can lead to correspondingly different results.
However, the different precision in the indications of the central corneal thickness also lead to measurement inaccuracies. While the Pentacam® AXL and the fiji program used for the analysis of the images taken by the intraoperative OCT can measure the corneal thickness with an accuracy of 1 µm, the Visante™ OCT rounds the values to an accuracy of 10 µm. The fact that an average value was calculated from three measurements made it possible to reduce this inaccuracy, but it is nevertheless reflected in the results in the form of a large standard deviation.
Central lens thickness
We found a large difference between the measured values of the lens thickness. The intraoperative OCT of the LenSx® laser shows a 0.96 mm thicker lens (median difference) than that measured by the Pentacam® AXL (mean difference -0.95 ± 0.58) (Table 1). This value is statistically significant and shows a clinically relevant difference. In addition to a possible measurement error between the two devices, a cause for this result could be the change in the lens radii, which occurs when the patient interface of the LenSx® laser is positioned on the patient's eye via suction. This was already observed in a 2009 study by Kunert et al.8 As a result of the suction, the radius of the front surface of the lens steepens. If this is also the case here, the result would be an increase in central lens thickness due to the steepening of the central radii of the eye lens.
However, the positioning of the test subject must also be taken into account. The measurement of the Pentacam® AXL was performed on a seated test subject, while the measurement of the intraoperative OCT was performed while the patient was lying down. It is possible that, as a result of the change in position from vertical to horizontal, the anterior segment of the eye changes and, hence, the lens becomes thicker. However, this effect has not yet been studied.
Furthermore, the data collection itself must be critically analysed. The images of the intraoperative OCT were measured manually with the help of a software program while the lens thickness of the Pentacam® AXL images was determined by internal software. The quality and resolution of the images differ greatly, whereby the Pentacam® AXL enables a finer image thanks to the Scheimpflug process. The eye lenses are often slightly tilted in the images of the intraoperative OCT. This is probably caused by the lying position and the suction of the patient interface. The manual measurement of the lens thickness at the pupil centre is therefore more difficult.
Conclusion
This study shows that there are clinically relevant differences between the measurement results of the intraoperative OCT of the LenSx® femtosecond laser, as well as the Pentacam® AXL and the Visante™ OCT.
The internal anterior chamber depth, measured with the intraoperative OCT of the LenSx® femtosecond laser, is smaller than the ACD measured with the other two methods. It is likely that the pressure of the patient interface on the anterior eye segment deforms the cornea. It is also possible that the pressure on the rigid, curved patient interface of the laser causes the cornea to change its curvature, which results in a modified anterior chamber depth. The comparison of Pentacam® AXL and Visante™ OCT shows that the devices deliver comparable results when it comes to the measurement of the internal anterior chamber depth. The procedures can thus be regarded as equivalent.
Due to the large spread of the measured values for the nasal and temporal chamber angles, no quantitative statement can be made about the influence of the patient interface on these parameters. The automatic chamber angle detection of the Pentacam® AXL has a high sensitivity and therefore does not always work correctly, especially with scattered light caused by a light iris. The device can consequently be used with certain restrictions as a comparative method. The Visante™ OCT software only allows for manual measurement of the chamber angles, which means that the subjectivity of the examiner can strongly influence the results. This can be avoided in future studies by using several examiners to evaluate the images.
The two comparative methods measure a lower corneal thickness than the intraoperative OCT, but the different measurement methods and resolution of the images represent a limitation of the results.
Clear differences between the procedures can be seen in the case of the central lens thickness. The Pentacam® AXL measures a smaller lens thickness compared to the intraoperative OCT. The difference in thickness can be traced back to the change in the patient's position from sitting to lying and to the suction of the eye through the patient interface.
The clinically relevant differences in the measurement results can also be due to possible measurement deviations of the devices. However, the reduction of the ACD measured by the intraoperative OCT indicates that the docking of the patient interface affects the anterior segment of the patient's eye.
Conflict of interest
The authors declare that there is no conflict of interests regarding the methods and devices mentioned in the article.
